Usually it's a good sign when you hear a patient coming through the ER with their shrieks echoing off the green tile walls, but with this one, there was a twist. The disheveled, emaciated gentleman was chanting, "I'm breaking a record. get me back up there." Strange indeed.
As I approached him, a strange combination of olfactory stimuli assaulted my prominent, sensitive beak, a sweet-sour miasma of cigarette smoke and Old Spice cologne to mask the imbedded dirt that made his skin look like a Jackson Pollack work of abstract art. The combination of different colored dirt and a panoply of greenish fungal lesions was a sight to behold.
I checked the skin turgor on an atrophied bicep and the little mountain of skin generated by the gentle pinch had the staying power of a member of the nurse academic/administrative office sitter complex ensconced in a Lazy Boy recliner. This poor soul was severely dehydrated.
Of course, in pre-EMS days, the Chicago Police were responsible for most patient transfers, and it was prudent to pay heed to the officer's admission commentary for a history of the patient's injury or treatment insights. The jolly young officer presenting us with our latest challenge had an unusual warning that really piqued our curiosity, "You better be able to rehabilitate this one or you're going to have to order a sitting 'em up coffin for him." Sure enough, the unveiling accomplished by an Abra Cadabra top sheet removal revealed some of the most severe lower leg contractures I have ever seen, with his knees flexed at a 45-degree angle so that a conventional flat, horizontal coffin would never accommodate him. This patient was a poster boy for the hazards of immobility.
No, this was not a nursing home patient. It was obvious from the poor soul's wrinkled, weathered, and deeply tanned skin that he had spent considerable time communing with the natural world in the good old outdoors. His well tan, wrinkled extremities had the color of tobacco juice and upon removing his tee shirt emblazoned with the slogan "ANGER MANAGEMENT PISSES ME OFF," a few scraggly chest hairs emerged from a chest that looked like the color of skim milk.
Perhaps a hiker who experienced a mishap on the trail or a construction worker? The patient was strangely nonverbal when queried about his plight, and as the mystery deepened, we decided that treating his dehydration would be a good place to start. His serum osmols were sky high and poor skin turgor cried out for hydration.
We lacked that clever whippersnappern vernacular back in the day, but the new fangled term "fluid resuscitation" described what was acutely needed here. Unfortunately, a cursory review of his arms revealed that finding a vein was going to be like looking for a black cat in a coal mine. I corralled the friendly resident to place a central line. He opted to place it in the subclavian vein running just below the clavicle. He punctured the big vein with ease and after verifying a good, nonpulsatile flow began threading the guide wire through the needle. After sliding the catheter in we were in business.
It didn't take long for our efforts to bear fruit and the poor soul began relating his adventurous, but misguided tale. He had been hired by a newly established whiskey distillery on Lincoln Avenue to set a flag pole sitting record as a publicity stunt. This activity, popular in the 1920s and resurrected in the 1960s was exactly as described. Our patient had been confined to a whiskey barrel platform erected on the very tip of a 60 foot flag pole. He was planning to break a 30 day record but was retired after several weeks when his ground crew could not communicate with him and called the Chicago police who delivered him to our ER.
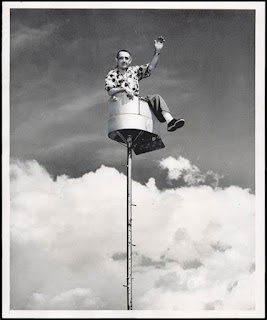 |
| What goes up, must come down |
Before internet advertising, business had to invent a number of whacky schemes to promote their ventures. Oscar Mayer company had a vehicle resembling a hot dog on 4 wheels aptly called the wienermobile and it was piloted by none other than Little Oscar. Car dealerships used high voltage floodlights to illuminate the night sky and bring in customers. Like the emaciated flag pole sitter some of these promotions ended in a trip to the hospital. Lincoln Mercury had a genuine Cougar on hand at Chicago's Ampitheater auto show and all was hunky dory until the beast attacked his trainer.
It's a good reason that hospitals were not allowed to advertise or I suspect misguided CEOs would have considered a nurse for flag pole sitting duty. They expected us to perform just about any unsavory or unpleasant task imaginable.
'
.png)
.jpg)









